
Keywords
Dieulafoy’s lesion
bleeding
colon
Abstract
We present a case report of recurrent bleeding from a Dieulafoy’s lesion in the cecum. This is a rare cause of bleeding into the lower gastrointestinal tract, clinically manifesting from minor to massive bleeding with the development of severe microcytic anemia requiring hospitalization and blood transfusion. Diagnosis and therapy are based on endoscopic examination of the lower digestive tract and are considerably limited by the intermittent nature of the bleeding, which often results in false negative findings. Treatment is based on achieving hemostasis utilizing endoscopic methods such as adrenaline injection, argon plasma coagulation, and using hemoclips. Only a few case reports of Dieulafoy’s lesions in the colon have been described in the available literature. Even though the lesion is rare, it is necessary to consider it in the differential diagnosis of anemia, especially in cases with negative results of the initial endoscopic examination.
This article is an English translation of the original Czech publication. The translation was generated with the assistance of artificial intelligence and has been reviewed and approved by the authors. The original version remains the authoritative source.
Introduction
Dieulafoy lesions are aberrant dilated submucosal arteries that erode the mucosa without ulceration and can lead to gastrointestinal bleeding [1]. The clinical picture ranges from mild, sometimes imperceptible, to massive, life-threatening bleeding. These lesions account for approximately 1–2% of all cases of bleeding into the digestive tract, with 80% of them located in the upper part. The incidence of symptomatic Dieulafoy lesions in the colon does not exceed 2% [2]. Localization in the cecum is very rare, with only a few cases reported [3]. The diagnosis of Dieulafoy lesions is often complicated by the intermittent nature of bleeding and their sporadic occurrence, which leads to frequent oversights even during endoscopic examination. Endoscopic methods of hemostasis are used for treatment – injection, thermal, and mechanical, or a combination thereof [4].
Case report
An 81-year-old female patient was referred by her general practitioner to the emergency department for anemic syndrome with severe normocytic anemia. The patient had a history of atrial fibrillation and was treated with apixaban at a dose of 10 mg daily. This was a repeat hospitalization with similar symptoms (after 11 and 10 months).
During her first hospitalization (9/2024), her hemoglobin level was 62 g/l at the time of admission. A differential diagnosis of anemia was performed, including abdominal ultrasonography, gynecological examination, and esophagogastroduodenoscopy. These examinations revealed no pathological findings. Colonoscopy was not indicated during the first hospitalization due to its recent performance at another facility with negative findings (1/2024).
One month after discharge, the patient was rehospitalized with similar symptoms, with an initial hemoglobin value of 71 g/l, without other pathological values in laboratory tests. A subsequent
colonoscopy revealed active punctate bleeding on the mucosal fold of the cecum, with calm surrounding mucosa and no defects (Fig. 1). The lesion was assessed as suspected angiodysplasia in the cecum and was treated with argon plasma coagulation (APC) to achieve hemostasis. During both hospitalizations, blood substitution was necessary, with a total of eight blood transfusions administered.
Ten months after this procedure, severe anemia developed again with a hemoglobin value of 72 g/L. The patient was admitted to our department and, after blood substitution and stabilization of her condition, a colonoscopy was indicated. The examination again showed active focal bleeding on the mucosal fold of the cecum, consistent with the previous colonoscopic examination (Fig. 2).
The finding was assessed as recurrent bleeding from a Dieulafoy lesion, which was treated with APC followed by the application of a safety hemoclip, achieving complete hemostasis (Fig. 3). During hospitalization, blood replacement therapy was administered with four blood transfusions.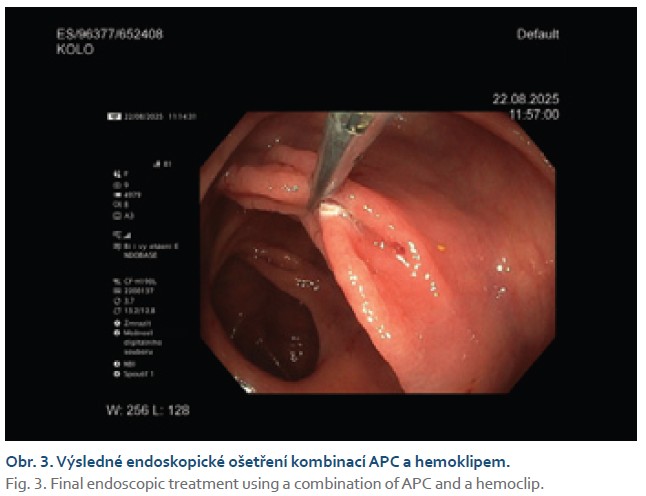
During the further course of hospitalization, the patient showed no signs of continued bleeding, no decrease in the hemogram in the control blood count, and the patient was discharged to outpatient care in a hemodynamically compensated state.
Discussion
Since its first description by Barbier in 1985, Dieulafoy's lesion remains a rare cause of bleeding in the lower gastrointestinal tract [5]. Diagnostic and therapeutic options are expanding with the development of endoscopic methods. CT angiography and erythrocyte scintigraphy with subsequent surgical resection, which were previously performed, have been abandoned in favor of endoscopic treatment, which is also in the current recommendations of the European Society of Gastrointestinal Endoscopy [6].
Dieulafoy lesions of the gastrointestinal tract are characterized by painless intermittent bleeding, which may manifest clinically as enterorrhagia or melena depending on its location, or may be completely clinically silent. In 70% of cases, the lesion occurs in the upper gastrointestinal tract and only approximately 2% in the large intestine. They mainly affect men (at a ratio of 2:1), most often in their fifth decade of life. Risk factors include arterial hypertension, chronic kidney disease, and cardiovascular disease, as well as the use of NSAIDs (non-steroidal anti-inflammatory drugs) and anticoagulant therapy (as in our case). There is no known genetic predisposition to the disease. The geographical distribution of the disease seems to mirror the availability and advancement of endoscopic methods, with the highest prevalence in the USA (32%), Japan (19%), and Korea (16%) [7].
Primary hemostasis can be achieved by endoscopic intervention using adrenaline injections, hemoclips, or argon plasma coagulation with a success rate of more than 90% [8]. Studies show that endoscopic methods maintain hemostasis for at least 6 months [9].
Similar to cases of Dieulafoy lesions in the stomach, cases of recurrent bleeding in the colon have also been described. If endoscopic methods fail, angiographic embolization or surgical treatment can be used as rescue therapy. There has even been a case report of combined therapy using arterial embolization followed by endoscopic laser coagulation as a last resort [10].
Our case report shows that the rarity of Dieulafoy lesions in the lower digestive tract can be problematic in the diagnostic process. During the first diagnostic colonoscopy in our patient, the
lesion was assessed as suspected angiodysplasia in the cecum due to the higher probability. Argon plasma coagulation was used to achieve hemostasis without combining it with a mechanical method, which is recommended for the treatment of Dieulafoy lesions, which may have contributed to the recurrence of bleeding [11]. Therefore, even though it is rare, it is important to consider the possibility of a Dieulafoy lesion as a source of bleeding in the lower gastrointestinal tract and to adapt the method of endoscopic hemostasis accordingly.
Conclusion
Dieulafoy lesions are among the less common causes of bleeding in the digestive tract. They predominantly occur in the upper gastrointestinal tract. Their occurrence in the colon is very rare, and the case report documenting recurrent severe bleeding from a Dieulafoy lesion in the cecum is unique. The rare occurrence and intermittent nature of bleeding can pose a diagnostic problem that may require repeated colonoscopy even in cases of initially negative findings.
ORCID autorů
P. Hříbek 0000-0002-8090-4389,
T. Grega 0000-0002-2490-8078,
Z. Vacková 0000-0002-0443-5752,
J. Csomor 0000-0002-8121-1170,
Š. Suchánek 0000-0003-3659-0252,
P. Urbánek 0000-0002-1506-1135.
Doručeno/Submitted: 27. 10. 2025
Přijato/Accepted: 19. 11. 2025
Korespondenční autor
MUDr. Petr Hříbek, Ph.D.
Interní klinika
1. LF UK a ÚVN – VFN Praha
U Vojenské nemocnice 1200/1
169 02 Praha 6
petr.hribek@uvn.cz
Literatura
1. Lee YT, Walmsley RS, Leong RW et al. Dieulafoy’s lesion. Gastrointest Endosc 2003; 58(2): 236–243. doi: 10.1067/mge.2003.328.
2. Khan S, Niaz S, Singh R et al. Dieulafoy lesion of the colon: a rare finding during colonoscopy. Cureus 2022; 14(5): e25188. doi: 10.7759/cureus.25188.
3. Dokmak A, Muso E. Gastrointestinal bleeding from Dieulafoy’s lesion in the cecum. Case Rep Gastroenterol 2022; 16(3): 601–606. doi: 10.1159/000525740.
4. Jeon HK, Kim GH. Endoscopic management of Dieulafoy’s lesion. Clin Endosc 2015; 48(2): 112–120. doi: 10.5946/ce.2015.48.2.112.
5. Barbier P, Luder P, Triller J et al. Colonic hemorrhage from a solitary minute ulcer. Gastroenterology 1985; 88(4): 1065–1068. doi: 10.1016/s0016-5085(85)80030-5.
6. Karstensen JG, Ebigbo A, Aabakken L et al. Nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) cascade guideline. Endosc Int Open 2018; 6(10): E1256–E1263. doi: 10.1055/a-0677-2084.
7. Inayat F, Hussain A, Yahya S et al. Rectal Dieulafoy’s lesion: a comprehensive review of patient characteristics, presentation patterns, diagnosis, management, and clinical outcomes. Transl Gastroenterol Hepatol 2022; 7: 10. doi: 10.21037/tgh.2020.02.17.
8. Baxter M, Aly E. Dieulafoy’s lesion: current trends in diagnosis and management. Ann R Coll Surg Engl 2010; 92(7): 548–554. doi: 10.1308/003588410X12699663905311.
9. Ma C, Hundal R, Cheng EJ. Colonic Dieulafoy’s lesion: a rare cause of lower gastrointestinal hemorrhage and review of endoscopic management. Case Rep Gastrointest Med 2014; 2014: 436293. doi: 10.1155/2014/436293.
10. Macrì A, Saladino E, Versaci A et al. Massive bleeding from a Dieulafoy’s lesion of the duodenum successfully treated with “adjuvant” transarterial embolization and endoscopic laser coagulation. Acta Chir Belg 2010; 110(2): 208–209. doi: 10.1080/00015458.2010.11680599.
11. Nojkov B. Distinctive aspects of peptic ulcer disease, Dieulafoy’s lesion, and Mallory-Weiss syndrome in patients with advanced alcoholic liver disease or cirrhosis. World J Gastroenterol 2016; 22(1): 446–466. doi: 10.3748/wjg.v22.i1.446.