
Keywords
laryngitis
extraintestinal manifestations
infliximab
ustekinumab
Abstract
Crohn’s disease is a chronic inflammatory disease affecting various locations of the gastrointestinal tract, sometimes involving other organ systems. The article illustrates a case of a patient who presented with an extremely rare laryngeal involvement in Crohn’s disease followed by a consecutive multidisciplinary therapeutic approach.
This article is an English translation of the original Czech publication. The translation was generated with the assistance of artificial intelligence and has been reviewed and approved by the authors. The original version remains the authoritative source.
Introduction
Crohn's disease is a chronic inflammatory disease belonging to the group of idiopathic inflammatory bowel diseases (IBD), affecting various parts of the digestive tract, from the oral cavity to the anus. According to the Swedish ICURE registry, Crohn's disease affects the large intestine in approximately 49% of patients, the terminal ileum in 28% of patients, ileocolonic involvement is present in almost 23% of patients, and the proximal gastrointestinal tract is affected in about 18% of patients [1].
In addition to gastrointestinal involvement, 5–50% of patients with IBD also experience extraintestinal manifestations (EIM). The most common EIM are musculoskeletal EIM, occurring in approximately 40% of patients with IBD. These EIMs include non-inflammatory arthralgia and peripheral arthritis, which are divided into pauciarticular (concordant with IBD activity) and polyarticular (discordant with IBD activity). They also include less common axial arthritis and spondyloarthritis, specifically ankylosing spondylitis (5–10% of IBD patients), sacroiliitis (25% of IBD patients), and inflammatory back pain. Dactylitis and enthesitis occur rarely [2,3].
The second most common EIMs are skin EIMs. They occur in approximately 15% of patients and include erythema nodosum, pyoderma gangraenosum, Sweet's syndrome (acute febrile neutrophilic dermatosis), and metastatic Crohn's disease of the skin. This subgroup consists also of lesions of the oral cavity, namely simplex aphthous lesions, periodontitis, pyostomatitis vegetans, and rare granulomatous cheilitis. Skin EIMs usually correlate with the activity of IBD itself in the gastrointestinal tract and relatively often precede IBD relapse [2,3].
Thirdly, the literature mentions ocular manifestations affecting approximately 2–5% of IBD patients, the most common of which are episcleritis and scleritis, similar to pauciarticular arthritis correlating with IBD activity in the gastrointestinal tract. In contrast, uveitis tends to be independent of IBD activity in the gastrointestinal tract and often precedes the actual manifestation of IBD [2,3].
Hepatopancreatobiliary EIMs include primary sclerosing cholangitis (PSC), autoimmune hepatitis, granulomatous hepatitis, IgG4-associated cholangitis, and autoimmune pancreatitis (type 2). From a certain point of view, concomitant metabolic diseases, such as hepatic steatosis, cholestatic hepatopathy, or accelerated formation of gallstones, caused by bile acid malabsorption in the terminal ileum, can be included among hepatopancreatobiliary manifestations. It can be difficult to distinguish between hepatic lesions caused by IBD itself and iatrogenic drug-induced damage [2,3]. More frequent occurence of oxalate nefrolithiasis is commonly found in patients after ileocecal resection or ileal dysfunction in Crohn´s disease. Intestinal resorption disorders also lead to a decrease in bone density (14–42% of patients with IBD). From a cardiovascular perspective, chronic inflammatory activity causes acceleration of atherosclerosis with subsequent effects on the cardiovascular system. During IBD relapse, the incidence of thromboembolic disease is several times higher [2,3].
There are only a few case studies documenting rare EIM cases involving respiratory, cardiovascular, and urogenital systems. Specific case studies describe pneumonitis, pulmonary granulomas, laryngitis, perimyocarditis, and glomerulonephritis [2–4].
Case study – Crohn's disease of the larynx
Laryngeal involvement is extremely rare. Only 15 cases have been documented in case studies to date worldwide [4].
A female patient born in 1965 was repeatedly examined outside our facility in 2003 for prolonged colitic syndrome. Initially, serological testing suggested yersiniosis. Empirical antibiotic treatment was ineffective, so a colonoscopy was performed, during which the finding in the large intestine was assessed as ulcerative colitis. However, during a subsequent endoscopic examination, skip lesions were identified and the finding was reevaluated as Crohn's disease of the large intestine. A CT scan of the abdomen was performed, revealing terminal ileitis. The patient was treated with repeated pulses of corticosteroids with the gradual development of corticosteroid dependence, for which azathioprine was added to the treatment in 2006 and a follow-up MR enterography examination was performed, which did not show any active inflammatory foci in the small intestine. In 2008, the patient underwent cholecystectomy for recurrent biliary colic with verified cholecystolithiasis.
In 2010, there was a relapse of colitic syndrome, and a colonoscopy revealed a relapse of Crohn´s disease of the large intestine, and the patient was referred to the IBD Center at the University Hospital in Trenčín. In November 2010, the patient began treatment with infliximab (IFX) at a standard dose of 5 mg/kg body weight i.v. every 8 weeks in combination therapy with azathioprine 100 mg daily. Despite the step-up in treatment, the patient experienced repeated relapses of polyarthralgia, so a follow-up colonoscopy was performed in early 2012, revealing pseudopolypoid changes in the right side of the colon. Staged biopsies histologically demonstrated moderate inflammatory activity, predominantly in samples from the right side of the colon. At the end of 2013, Crohn's disease relapsed in the perianal area, requiring surgical and antibiotic treatment. A supplementary MR scan of the small pelvis showed no fistulas or further abscesses. An endoscopic examination of the sigmoid colon (due to the patient's intolerance to the examination) revealed a relapse of Crohn's disease in the sigmoid colon as well. In view of these findings, the patient's IFX dose was increased to 10 mg/kg i.v. every 8 weeks in March 2014 (IFX and antidrug antibody levels were also tested, but the results are missing from the archived documentation). In December 2014, due to anaemia and weight loss, an abdominal CT scan with colonography was performed, among other tests, describing the already known polypoid formations in the cecum. Since the summer of 2015, the patient has experienced repeated relapses of arthralgia 6 weeks after infliximab administration, which led to a reassessment of the IFX therapeutic strategy to 5 mg/kg i.v. every 6 weeks. However, even after the treatment adjustment, there was no remission of polyarthralgia. In April 2016, an allergic reaction occurred during IFX infusion therapy, after which IFX administration was immediately discontinued and adalimumab (ADA) 40 mg s.c. every 14 days was added to the treatment. In October 2017, MRCP was performed due to transient cholestasis, with no findings suggestive of PSC.
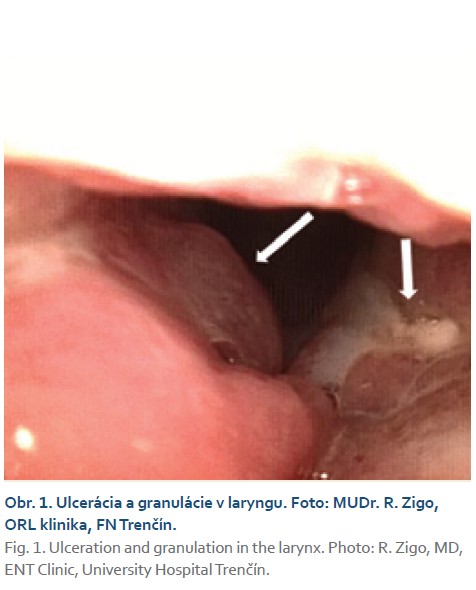
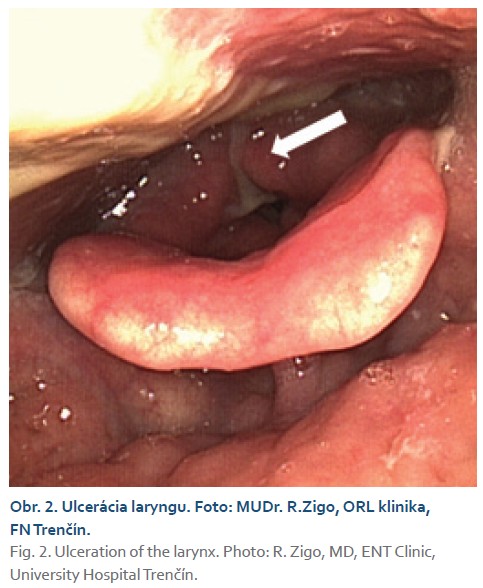
Treatment with ADA in combination with azathioprine 100 mg daily resulted in alleviation of polyarthralgia, but not complete remission. The patient's condition was stable for approximately 4 years, with no relapse of Crohn's disease in the digestive tract. In March 2020, during a check-up, the patient complained of significant hoarseness, phlegm, odynophagia, and coughing lasting several weeks. The condition was assessed by an otolaryngologist as acute pharyngitis, and the patient was empirically prescribed antibiotics and local treatment. A culture test from the pharynx did not detect any pathogens. Due to the progression of the symptoms, a laryngofibroscopic examination was performed, which revealed granulomatous laryngopharyngitis (Figs. 1, 2). The histological findings were assessed by a pathologist as consistent with Crohn's disease in the larynx. Despite local therapy, the condition progressed and in June 2020, hospitalization with high doses of parenteral corticosteroids was necessary, which led to significant relief of pharyngeal symptoms. The ADA trough level was 8.2 μg/ml.
After stabilization of the condition and partial reduction of the corticosteroid dose, a switch to ustekinumab in combination with azathioprine 100 mg daily was indicated in the patient from August 2020. Over the course of 3 months, with further gradual reduction of the corticosteroid dose, there was complete resolution of throat pain and hoarseness and almost complete resolution of arthralgia. Over the next 5.5 years, while continuing treatment with ustekinumab 90 mg s.c. every 12 weeks, the patient remained in clinical remission of both colitic and laryngeal symptoms, fecal calprotectin was repeatedly low (in the negative range), and joint EIM occurred only sporadically, significantly less frequently than with conventional and anti-TNFa treatment. In April 2025, a follow-up colonoscopy was performed, revealing endoscopic and histological remission of Crohn's disease in staged biopsies from the terminal ileum and segments of the large intestine. A follow-up laryngofibroscopy also showed only minimal changes in the laryngeal mucosa, with no relapse of laryngeal EIM (Fig. 3).

Discussion
Crohn's disease of the larynx is a rare extraintestinal manifestation of this disease. Symptoms of Crohn's disease affecting the larynx include hoarseness, dyspnea, sore throat, and odynophagia. Local findings in the larynx include edema, erythema, ulceration, and granulation [4].
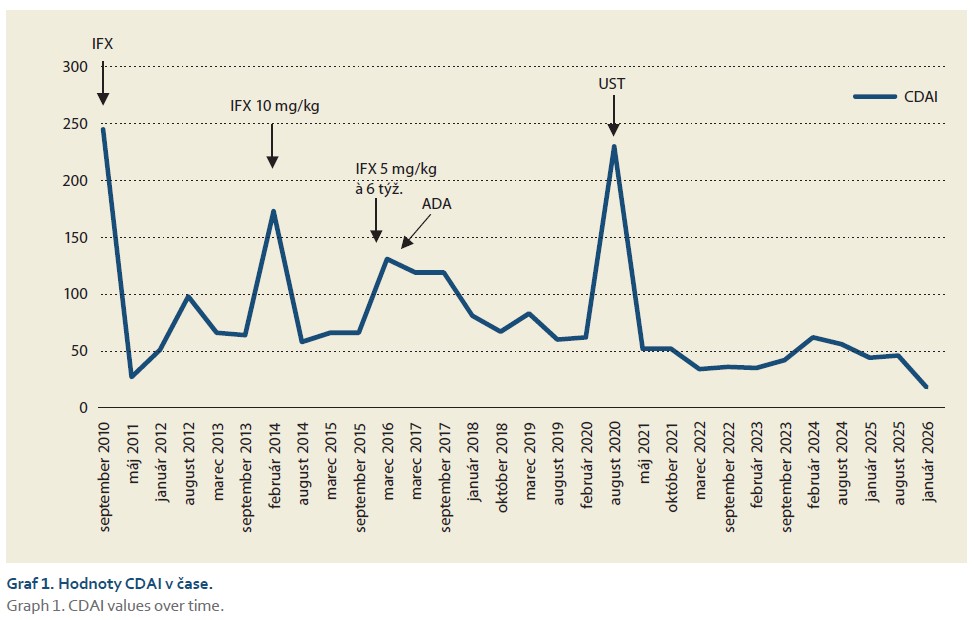
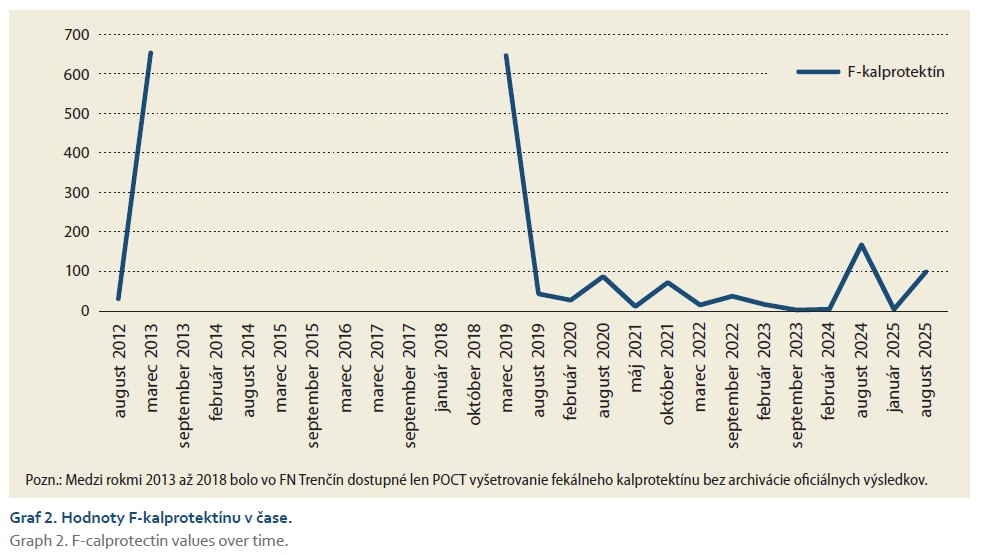
Given the immunomodulatory treatment administered, it is necessary to consider opportunistic fungal or mycobacterial pathogens and other autoimmune diseases (sarcoidosis, granulomatosis with polyangiitis) in the differential diagnosis of patients with IBD, in addition to common infectious or neoplastic diseases. Of course, it is necessary to perform histology of all available lesions and thoroughly complete the request form for histopathological examination. Treatment of laryngeal manifestations of Crohn's disease involves the administration of high doses of corticosteroids with a transition to another type of innovative IBD treatment [4]. Figures 1 and 2 show the development of CDAI and F-calprotectin values during the treatment of the patient at our facility. CDAI values reflect the patient's clinical condition, whereas F-calprotectin values, despite the involvement of the large intestine, do not reflect the severity of the condition and their use was therefore limited.
Conclusion
Extraintestinal involvement of the larynx by Crohn's disease is rare. Identification and association of symptoms with the underlying diagnosis are key to further patient management. In rare complications of the disease, communication between specialists and a multidisciplinary approach to patient care are essential.
Doručené/Submitted: 20. 1. 2026
Prijaté/Accepted: 28. 1. 2026
Korespondenčný autor
MUDr. Milan Hlista
Gastroenterologická ambulancia
FN Trenčín
Legionárska 594/28
911 01 Trenčín
milan.hlista@fntn.sk
Literatúra
1. Bureš J, Lukáš M. Idiopatické střevní záněty. In: Zavoral M (ed). Mařatkova gastroenterologie: patofyziologie, diagnostika, léčba. Praha: Karolinum 2021: 646–701.
2. Malik TF, Aurelio DM. Extraintestinal manifestations of inflammatory bowel disease. Treasure Island (FL): StatPearls Publishing 2025.
3. Rogler G, Singh A, Kavanaugh A et al. Extraintestinal manifestations of inflammatory bowel disease: current concepts, treatment, and implications for disease management. Gastroenterology 2021; 161(4): 1118–1132. doi: 10.1053/j.gastro.2021.07.042.
4. Yin X, Zhu J, Zheng Y et al. Laryngeal involvement in a patient with Crohn‘s disease: a case report. Asian J Surg 2023; 46(3): 1334–1335.