
Keywords
quality of life
Crohn’s disease
ulcerative colitis
biological products
patient reported outcome
measures
depression
employment
Abstract
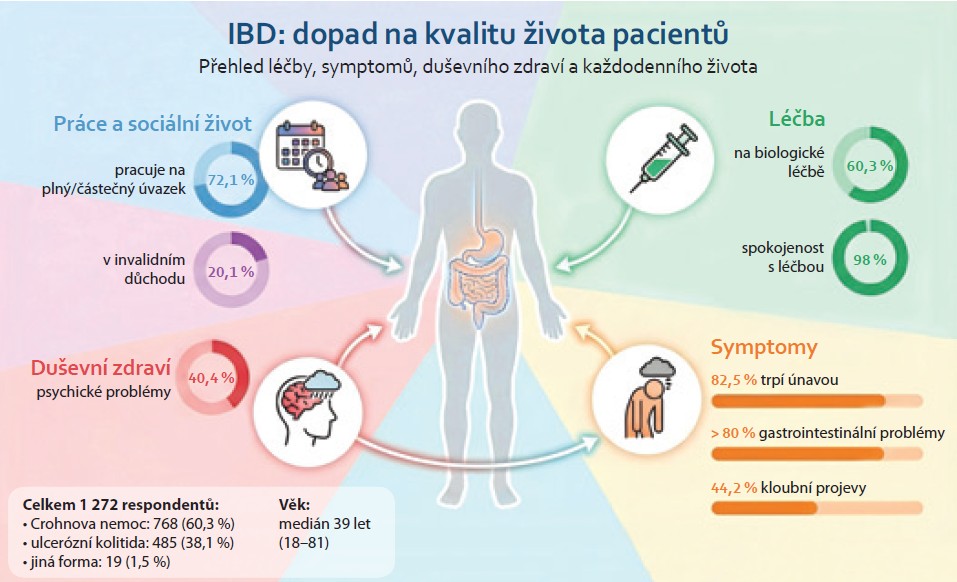
Introduction: Normalization of the quality of life is an important therapeutic goal in patients with inflammatory bowel disease (IBD). Aim: To evaluate the quality of life in patients with IBD in the Czech Republic. Methods: The study involved patients with IBD aged ≥ 18 years who were approached through gastroenterology departments in the Czech Republic and online through a patient organization. Patients completed a one-time, anonymous questionnaire focusing on various aspects of the quality of life. Results: The study was conducted between September 2024 and May 2025 involving 1,272 patients (60% with Crohn‘s disease, 58% women, median age 39 years, and 60.3% on biological therapy). The most commonly reported problem associated with IBD was fatigue (82.5%), followed by gastrointestinal symptoms and extraintestinal manifestations. Up to 40% of respondents reported psychological problems (anxiety and depression). Approximately two-thirds of patients (57–69%) admitted to at least occasional restrictions in social activities such as travelling, playing sports, or eating in public places. Two-thirds of respondents (72.1%) stated that they work full-time or part-time, and 20.1% admitted to receiving disability pension. Targeted therapy – biologics and small molecules (OR 1.74; 95% CI 1.25–2.45), Crohn‘s disease (OR 1.48; 95% CI 1.09–2.03), and relapse frequency ≥ 1 per year (OR 2.73; 95% CI 2.02–3.72) increased the risk, while higher education (OR 0.48; 95% CI 0.34–0.66) reduced the risk of disability. Conclusion: This study highlighted the negative impact of IBD on various aspects of patients‘ lives, particularly their personal and professional lives, and the high incidence of mental health problems among IBD patients.
This article is an English translation of the original Czech publication. The translation was generated with the assistance of artificial intelligence and has been reviewed and approved by the authors. The original version remains the authoritative source.
Introduction
Inflammatory inflammatory bowel diseases (IBD) is a chronic, medically incurable disease that is mainly diagnosed in young adults. While the life expectancy of patients with IBD is comparable to that of the general population, existing studies point to a significant negative impact of the disease on the quality of life of patients, leading to disability in some cases [1]. Normalizing quality of life and preventing disability are among the long-term therapeutic goals for patients with IBD, as defined by an international group of experts on IBD [2,3]. In 2018, an extensive questionnaire survey focusing on the quality of life of patients with IBD in the Czech Republic was published, which was initiated by the patient organization Pacienti IBD z.s. [1]. This survey highlighted the negative impact of IBD on the quality of life of patients in the Czech Republic and their ability to work. In recent years, however, there have been relatively significant changes in the treatment options for IBD, both in terms of expanding the therapeutic spectrum with new drugs with different mechanisms of action as well as greater availability of effective, predominantly biological treatment for patients with IBD.
The aim of this study was to evaluatethe quality of life of patients with IBD in the Czech Republic. in light of the latest developments in the treatment options for IBD.
Methodology
The study was initiated by the patient organization Pacienti IBD z.s. in cooperation with representatives of the Working Group for Inflammatory Bowel Diseases of the Czech Gastroenterological Society of the Czech Medical Association, which brings together physicians interested in these diseases. It was a questionnaire survey following up on the original survey conducted in 2016 [1].
Patients
Patients with IBD aged 18 years and older participated in the study. Patients were contacted through gastroenterology centers in the Czech Republic and online through the patient organization. The patients completed a one-time, anonymous questionnaire focused on various aspects of quality of life in online (most respondents) or paper form.
Data collection
The questionnaire survey was conducted between September 2024 and May 2025. The questionnaire was based on the structure of the questionnaire from the previous study and was updated. It included a total of 52 questions divided into five areas focusing on:
a) patient demographic data;
b) IBD diagnosis and treatment;
c) the impact of the disease on quality of life;
d) the impact of the disease on work;
e) awareness of IBD.
Most of the questions and answers (49; 92%) were designed in the form of predefined answers with a choice of one or more options.
Statistical analysis
The analysis was performed using IBM SPSS Statistics and R (version 4.4.3, 2025-02-28 ucrt) with the tidyverse package for data manipulation and ggplot2 for visualization, and IBM SPSS Statistics (version 27). Associations between categorical variables were evaluated using the chi-square test and Fisher's exact test. Odds ratios were set with 95% confidence intervals (95% CI). Multivariate analysis was performed using logistic regression. The level of statistical significance was set at p < 0.05.
Results
The questionnaire survey was conducted in all 14 regions of the Czech Republic. Most of the respondents were treated at Prague centers (54.6%), followed by the South Moravian (7.9%) and Hradec Králové (6.4%) regions (Table 1).
A total of 1,272 patients with IBD participated in the study, 768 with Crohn's disease (CD) and 485 with ulcerative colitis (UC). Women slightly predominated (733; 57.6%), and the median age of respondents was 39 years.
The demographic and clinical data of the patients are shown in Table 1.
Treatment and adherence to treatment
At the time of the survey, 60.3% of respondents were receiving biological treatment, 3.9% were receiving treatment with small molecules, and 16.7% were receiving corticosteroids (Table 1). Almost all patients were completely (72.5%) or partially (25.6%) satisfied with their current treatment, and only 2% of patients expressed dissatisfaction. The results did not differ between patients with CD and UC (dissatisfaction 1.8% in CD and 1.9% in UC). Almost one-third of patients admitted to at least occasionally missing a dose/application of medication (28.4% with CD and 35.1% with UC). For most of them, the reason was forgetfulness (87%), while 8.1% of patients did not take their medication intentionally.
Most respondents reported that they had the option of consulting a gastroenterologist at their healthcare facility (86.2%). Some patients also reported that they had the option of consulting a rheumatologist (20.0%), dermatologist (21.9%), surgeon (22.2%), or nutritionist (27.3%). The availability of a psychologist was minimal, at 11.6% of cases. The vast majority of patients (93.3%) had access to treatment at their healthcare facility within 72 hours in the event of acute problems.
Impact of the disease on quality of life
The most frequently reported problem associated with the disease that bothered IBD patients was fatigue (82.5%), followed by gastrointestinal problems (diarrhea 81.1%; abdominal pain 74.7%; urgency 69.3%; bleeding 50.7%; and tenesmus 48.4%). Almost half of the respondents (44.2%) also reported joint problems and 41.7% reported skin manifestations related to the disease or as a complication of treatment (Figure 1a). The frequency of problems differed between patients with CD and UC. While fatigue followed by gastrointestinal symptoms dominated in patients with CD, the most frequently reported problem in patients with UC was diarrhea, followed by fatigue and urgency (Figures 1b, c).
Up to 70% of patients had to change their personal plans at least once in the last six months due to intestinal disease, and in 22.9% of cases this occurred frequently or very frequently (≥ 5 times). Most respondents (54–69%) reported at least occasional concerns about eating in restaurants, traveling on vacation, or traveling by public transport, or reported limitations in sports activities. On the contrary, IBD did not represent any limitation in establishing or maintaining relationships for most respondents (66.4%) (Table 2).
Anxiety or depression was reported by 40.4% of patients (39.1% with CD and 42.3% with UC); 13.5% reported regular treatment and 9.3% reported occasional treatment for these mental health problems. In univariate analysis, female gender (OR 1.84; 95% CI 1.46–2.32), disease activity (OR 2.09; 95% CI 1.61–2.71), and dissatisfaction with treatment (OR 4.81; 95% CI 1.91–12.13) were associated with a higher risk, while low relapse frequency (< 1× per year) was associated with a lower risk of these mental health problems (OR 0.48; 95% CI 0.38–0.60). The type of IBD (CN or UC) or the patients' ability to work had no effect. In multivariate analysis, IBD activity (OR 1.56; 95% CI 1.16–2.10) increased, while low relapse frequency decreased (OR 0.61; 95% CI 0.45–0.84) the risk of anxiety or depression.
Impact of the disease on work
Two-thirds of respondents (917; 72.1%) reported working full-time (664; 52.2%) or part-time (253; 19.9%), while 69 (5.4%) patients were already retired. One-fifth of respondents (256; 20.1%) reported receiving disability benefits. Patients treated with targeted therapy—biologics or small molecules (OR 1.52; 95% CI 1.12–2.07) and patients with CD (OR 1.48; 95% CI 1.10–1.99) had a higher risk of disability in the univariate analysis, while this risk was reduced by higher education (OR 0.44; 95% CI 0.32–0.60) and a lower frequency of IBD relapses (OR 0.36; 95% CI 0.27–0.48). In the multivariate model, targeted therapy (OR 1.74; 95% CI 1.25–2.45) and CD (OR 1.48; 95% CI 1.09–2.03) were associated with a higher risk, while higher education (OR 0.48; 95% CI 0.34–0.66) and lower relapse frequency (OR 0.37; 95% CI 0.27–0.49) were associated with a lower risk of disability.
More detailed data on the impact of the disease on the work capacity of patients with IBD was provided by 1,052 respondents. At least 1 day of work was missed in the last year due to IBD by 650 (61.8%) patients, and in 104 (9.9%) patients it was even more than 60 days. In univariate analysis, disease activity (OR 1.95; 95% CI 1.43–2.65) and targeted therapy increased the risk of work absence (OR 1.50; 95% CI 1.15–1.95), while low relapse frequency (OR 0.56; 95% CI 0.44–0.73) reduced this risk. IBD type and satisfaction with treatment were not statistically significantly associated. In the multivariate model, targeted therapy (OR 1.49; 95% CI 1.12–1.99) and disease activity (OR 1.66; 95% CI 1.18–2.37) were associated with a higher risk of missed workdays, while low relapse frequency (OR 0.67; 95% CI 0.50–0.90) was associated with a lower risk.
Most patients (685; 65.1%) had at least one period of sick leave due to IBD, of which 246 (23.4%) took sick leave more than six times.
Patients with CD had a higher risk of sick leave compared to patients with UC (OR 1.33; 95% CI 1.01–1.74). Similarly, targeted therapy (OR 1.49; 95% CI 1.12–2.00), the presence of extraintestinal manifestations (OR 2.08; 95% CI 1.59–2.72), and active disease (OR 1.58; 95% CI 1.1–2.1) increased the risk of sick leave, while a low frequency of relapses (OR 0.57; 95% CI 0.44–0.75) reduced the risk. In multivariate analysis, CN (OR 1.34; 95% CI 1.01–1.77), use of targeted therapy (OR 1.43; 95% CI 1.05–1.94), presence of extraintestinal manifestations (OR 1.9; 95% CI 1.45–2.50), and a higher frequency of relapses (OR 1.75; 95% CI 1.33–2.29) increased the risk of sick leave .
In the case of acute problems related to IBD, one-third of patients (419; 32.9%) deal with reduced work performance by taking sick leave, 268 (21.1%) by taking vacation, 416 (32.7%) by working from home, and 501 (39.4%) by agreement with their employer.
Most patients (71.4%) also reported feeling stressed or under pressure at work due to their illness, and approximately half of those surveyed (52.6%) were forced to adjust their work schedule. The impact of the disease on other aspects of working life is shown in Table 3.
Awareness of IBD
The vast majority of respondents (1,147; 90.2%) said they had sufficient information about IBD, including treatment options. The most common sources of information cited by patients were their treating physician (90.8%), self-study (74.1%), or the patient organization Pacienti IBD z.s. (37.7%).
Discussion
This paper presents an extensive survey focused on quality of life of patients with IBD in the Czech Republic and follows up on the previous survey conducted almost 10 years ago. The study pointed to the negative impact of IBD on various aspects of patients' lives, especially personal and work life. Furthermore, a significant number of patients have reported psychological problems such as anxiety or depression. . The results are comparable in many respects to the results of the previous survey.
Compared to the previous survey, more than half of the patients (60.3%) who participated in the current study were receiving biological therapy or small molecule therapy, compared to 31% of patients in the previous study [1]. The proportion of patients on systemic or topical corticosteroid therapy was lower in the current survey (16.7% vs. 30.9%). Otherwise, the patients did not differ significantly in terms of demographic and clinical characteristics. The shift towards a higher proportion of biological treatment in the current group of patients may reflect the expansion of the therapeutic spectrum and a change in treatment paradigms towards earlier, more intensive control of inflammation with advanced anti-inflammatory therapy – biological treatment or small molecules. It has been shown that initiating biological therapy early after diagnosis of CD increases the chance of achieving remission and is also cost-effective [4]. However, the high proportion of patients treated with advanced therapy in this study may also be influenced by the higher participation of centers providing biological therapy. . One thing that can be viewed as clearly positive- is the high proportion of patients satisfied with their treatment (98%).
Despite advances in the treatment of IBD, the symptomatic burden on patients remains high. As expected, gastrointestinal symptoms were reported as one of the most common. An exceptionally high number of respondents (83%) reported problems with fatigue, similar to a previous study [1]. Fatigue is a complex symptom, probably of multifactorial etiology, which is not directly proportional to the severity of intestinal inflammation, often persists even in patients in clinical remission an is usually difficult to treat [5]. Extraintestinal symptoms, especially joint symptoms, followed by skin and eye symptoms, were also frequently reported. These manifestations can significantly contribute to reduced work capacity and social activities and point to the need for a multidisciplinary approach in the care of patients with IBD. A significant and somewhat alarming finding was the high prevalence of anxiety and depressive symptoms, affecting up to 40% of respondents. Active disease was associated with a 2.5-fold higher risk of these mental health problems compared to quiescent disease, suggesting that disease activity remains an important determinant of not only physical but also mental health in patients [6]. The mechanisms of this relationship are multifactorial and include both the direct impact of somatic symptoms (pain, diarrhea, urgency, fatigue) and the psychosocial stress associated with disease relapse, sleep disturbance, and concerns about the future course of the disease. In addition, biological mechanisms also play a role through the action of inflammatory mediators and dysregulation of the gut-brain axis, which contribute to the development of depression and anxiety [7]. However, limited access to psychological care in clinical practice remains a serious problem, as highlighted by the results of our study, where only 12% of respondents had access to a psychologist at their center. Similar to the previous study, IBD had a negative impact on various aspects of respondents' private and social lives in the form of having to change private plans due to illness, concerns about eating in public dining establishments, concerns about traveling by public transport or going on vacation, and limitations in sports activities. Almost two-thirds of respondents reported at least occasional limitations in the above-mentioned activities. The high symptomatic burden observed in our respondents probably contributes to this unfavorable situation. On the other hand, a somewhat positive result is that most respondents had no (66%) or only occasional (20%) difficulties in establishing or maintaining romantic relationships.
IBD is associated not only with high direct costs, but also with indirect economic costs in the form of reduced work capacity or productivity or disability [8]. The significant negative impact of IBD on work capacity is also evidenced by data from our survey, which points to a significant proportion of respondents who reported the need for sick leave or absence from work due to their illness. The proportion of patients working full-time or part-time was slightly higher than in the previous study (72% vs. 66%). However, the current respondents show a deterioration in their professional quality of life in terms of more frequent feelings of stress at work due to their illness (71% vs. 38%), the impact of IBD on their choice of work (47% vs. 38%), or the need to adjust their work schedule due to IBD (53% vs. 42%). The proportion of respondents who reported receiving disability benefits was also slightly higher than in the previous survey (20% vs. 11%). An interesting and clinically relevant finding is the relationship between targeted therapy and disability. Biological treatment and small molecule treatment were associated with a higher risk of disability in multivariate analysis. This finding is likely to reflect the relationship between the severity of the disease, for which advanced therapy is indicated, and which leads to disability in some patients due to the complicated and refractory course of the disease. This is supported by the finding of a relationship between the frequency of relapses and the risk of disability in our respondents. Similarly, CD was associated with a higher probability of disability compared to UC. This result corresponds to the known differences in the natural course of both diseases [9]. Conversely, higher education was associated with a lower risk of receiving disability benefits, which is a common phenomenon in other diseases as well [10].
Disease activity was also associated with a higher risk of absenteeism (number of days missed/sick leave), as was the presence of extraintestinal manifestations. This finding demonstrates the importance of achieving disease remission with regard to patients' ability to work.
A positive finding of this study is the high level of patient awareness of their disease and treatment, which was reported by the vast majority of respondents (90% of respondents vs. 94% in the previous survey). The reported sources of information were heterogeneous; in addition to medical specialists, self-study and education through the patient organization, which is an important source of information and support for patients with IBD in the Czech Republic, played a significant role.
The main limitation of the study is the potential bias in the results due to the possible selection of a certain group of patients who participated in the survey. Therefore, our results cannot be automatically applied to the entire population of IBD patients in the Czech Republic. Another limitation is the uneven geographical representation of centers from individual regions in terms of patient sample size. Given that this is not an unselected sample of patients with IBD, it is difficult to assess the relationship between the higher prevalence of targeted therapy in current survey and changes in various aspects of patients' quality of life. Due to the nature of data collection, we cannot guarantee the accuracy of data on disease characteristics, such as the type of treatment and course of IBD with regard to the assessment of activity and frequency of relapses.
However, the strength of this study is the size of the patient population and the effort to represent the centers in all regions. Furthermore, we sought to take a comprehensive approach in this survey, covering various aspects of patients' lives in the psychosocial and socioeconomic spheres.
In conclusion, despite general progress and advances in the treatment of IBD, the results of our survey point to the continuing negative impact of the disease on the quality of life of IBD patients and their ability to work. The relatively high incidence of mental health problems in the respondent population and the negative impact of disease activity on the mental health point to the need to improve the availability of psychological care and, in particular, the need for effective and adequate treatment of active disease.
Acknowledgements
We would like to thank all doctors and nurses from IBD biological treatment centers and other gastroenterology departments who spread awareness about the questionnaire survey and distributed it to patients to fill out.
ORCID
P. Mináriková 0000-0001-6636-9335,
P. Matějková 0009-0002-3724-3631,
I. Kuzko 0009-0003-2638-6378,
D. Ďuricová 0000-0002-6090-3522.
Submitted: 7. 2. 2026
Accepted: 12. 2. 2026
Corresponding author
MUDr. Dana Ďuricová, Ph.D.
Clinical and Research Center for Inflammatory Bowel Diseases, ISCARE a.s.
and First Faculty of Medicine, Charles University, Prague
Českomoravská 2510/19
190 00 Praha 9
dana.duricova@seznam.cz
References
1. Ďuricová D, Pfeiferová M, Bortlík M et al. Kvalita života pacientů s idiopatickými střevními záněty v České republice – multicentrická studie. Gastroent Hepatol 2018; 72(1): 11–19. doi: 10.14735/amgh201811.
2. Le Berre C, Ricciuto A, Peyrin-Biroulet L et al. Evolving short and long term goals of management of inflammatory bowel disease: getting it right, making it last. Gastroenterology 2022; 162(5): 1424–1438. doi: 10.1053/ j.gastro.2021.09.076.
3. Turner D, Ricciuto A, Lewis A et al. STRIDE II: an update on selecting therapeutic target in inflammatory bowel disease (STRIDE) Initiative of International Organization for the study of IBD (IOIBD): determining therapeutic goals for treat-to-target strategies in IBD. Gastroenterology 2021; 160(5): 1570–1583. doi: 10.1053/j.gastro.2020.12.031.
4. Noor N, Lee J, Bond S et al. A biomarker-stratified comparison of top-down versus accelerated step-up treatment strategies for patients with newly diagnosed Crohn’s disease (PROFILE): a multicentre, open-label randomised controlled trial. Lancet Gastroenterol Hepatol 2024; 9(5): 415–427. doi: 10.1016/S2468-1253(24)00034-7.
5. von Arnim U, Scholz K. Fatique in inflammatory bowel disease. Best Pract Res Clin Gastroenterol 2025; 78: 102059. doi: 10.1016/j.bpg.2025.102059.
6. Barberio B, Zamani M, Black CJ et al. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: a systemic review and meta-analysis. Lancet Gastroenterol Hepatol 2021; 6(5): 359–370. doi: 10.1016/S2468-1253(21)00014-5.
7. Gracie DJ, Hamlin PJ, Ford AC. The influence of the brain-gut axis in inflammatory bowel disease and possible implications for treatment. Lancet Gastroenterol Hepatol 2019; 4(8): 632–642. doi: 10.1016/S2468-1253(19)30089-5.
8. Burisch J, Zhao M, Odes S et al. The cost of inflammatory bowel disease in high-income settings: a Lancet Gastroenterology & Hepatology Commission. Lancet Gastroenterol Hepatol 2023; 8(5): 458–492. doi: 10.1016/S24 68-1253(23)00003-1.
9. Dolinger M, Torres J, Vermeire S. Crohn’s disease. Lancet 2024; 403(10432): 1177–1191. doi: 10.1016/S0140-6736(23)02586-2.
10. Česká správa sociálního zabezpečení. 2025 [online]. Dostupné z: www.cssz.cz.